MBBS COVID Information
Section outline
-
-
-
Welcome to this e-learning module on Covid-19 vaccine hesitancy. We estimate it should take no more than 60-90 minutes, but you can do it in chunks
It's designed specially for medical and PA students, but will be useful for all health professionals who are involved in having discussions with patients who may be hesitant about having the Covid-19 Vaccine.
It has been developed with input from the local community in East London and students & faculty from the Institute for Health Science Education
The key approach we are using is based on best practice in communication skills and an evidence-based technique called "motivational interviewing"
-

-
-
-
-
-
-
People who are vaccine hesitant are uncertain about getting vaccinated, but remain open to it if they are convinced that vaccines are safe, effective, and necessary.
It's normal for people to hesitate when making important decisions. Having a new vaccine like the Covid vaccine is an important decision. Having the Covid vaccine is not mandatory.
It's important to distinguish between people who are "vaccine hesitant" and people who refuse all vaccines or are so-called "vaccine deniers" or "anti-vaxxers". ["Anti-vaxxer" is a term in common use; but feedback from the local community suggests that it can come over as extremely judgemental, and it's best not to use it when talking with or about patients]
Between those who are happy to accept all vaccines, and those who refuse all vaccines, there is a spectrum of different attitudes to having vaccines.
See the diagram below from The World Health Organisation: the "vaccine hesitancy continuum" outlines the range of attitudes among people who are vaccine hesitant. Note the tiny proportion of people who are "vaccine deniers" or "vaccine refusers".

-
Students mustView
An important step in talking to people about vaccine hesitancy is to establish where they are on the spectrum of attitudes towards having the Covid vaccine.
In this exercise, you are asked to match the patients to the most appropriate descriptions of where they are on the vaccine hesitancy scale
-
-
-
WHY ARE PEOPLE VACCINE HESITANT?
People are vaccine hesitant for a wide variety of reasons. But they broadly fall into three main categories:
Complacency [ie a feeling that the risk of disease is low for the individual concerned; or other things more important]
Confidence [eg lack of trust in the safety of vaccine, or in institutions or governments promoting it]
Convenience [perceived or real problems with accessing the vaccine, or for medical reasons]
-
Students mustView
Have a look at this visual summary of common concerns about Covid Vaccines and some tips on addressing them and links to great resources. Follow the sections in order: 1-5.
258.3 KB -
Students mustView
A brief editorial from BMJ exploring why some ethnic groups are more likely to be vaccine hesitant, and how we can try to tackle it
462.9 KB -
Students mustView
Barely a month into England's coronavirus vaccine programme, a stark inequality began to reveal itself. Black people were less likely than any other group, and half as likely as white people, to have had the jab.
By April 2021 , 64% of black over-50s had been vaccinated compared with 93% of white people of the same age. The reasons for this are complex. Unethical medical treatment in the past, ongoing discrimination and personal experiences of insensitive treatment by the NHS are all believed to play a part.
But doctors, researchers and campaigners who spoke to the BBC said they feared black communities were being blamed.
-
-
Students mustViewMake forum posts: 1
Please post a brief comment to share with other learners. Click on "reply" below to post your thoughts. Please answer these 2 questions in your post:
1. What is your role in these conversations? Please post a sentence or two describing what you think your role is when you talk with someone who is hesitant about having the Covid Vaccine. What are you trying to achieve?
2. How do these conversations make you feel? You may also wish to share a few thoughts about how these conversations make you feel; or how you imagine they might make you feel. Are you anxious, frustrated, angry, excited?
-
A PATIENT-CENTRED APPROACH
It's common for health professionals to feel their role here is to convince patients to take the vaccine, and perhaps correct any misunderstandings about the vaccine. Success would then be the patient changing their mind and accepting the vaccine.
This approach is understandable, but can often backfire and set up confrontation and lack of trust. Conversations aimed mainly at changing minds or correcting misinformation can become very doctor-centred, can seem disrespectful of patients' concerns and values [whether you think they are rational or not], and risk breakdown of rapport and trust.

Accurate information is crucial of course, but as we have seen, people make decisions about whether or not to have a vaccine based on so much more than simple information. All sorts of things influence peoples' choices, from their trust of institutions and health professionals, previous experiences and access, to perceptions of risk, friends and family opinions, and what they have read or seen.
Best practice and motivational interviewing techniques suggest that it is often more fruitful to adopt a more patient-centred approach, starting with listening to and respecting the patient's concerns :

Having listened respectfully to the patient's concerns, you are then in a good position to find out how you might be able to help them make the right decision for them.
-

Professor Stephen Rollnick, co-developer of motivational interviewing technique
-
-
How to have the conversation
If your patient is happy to accept the vaccine, then you can offer positive encouragement and administer the vaccine as you would normally.
If your patient is adamantly refusing, or perhaps is an "anti-vaxxer", don't get into a heated debate. Listen to their concerns, leave space for further discussion, and offer to refer to other health professionals if they would find that helpful. It is important however that patients are aware of the consequences and responsibilities of not having the vaccine (eg transmission risks, risks of illness, need for healthcare), and this is recorded in their notes.
But for all vaccine hesitant patients, consider an approach using principles of motivational interviewing.

-
SUMMARY OVERVIEW OF KEY SKILLS
Using a mix of best practice in clinical communication skills and motivational interviewing, this is a step-by-step overview of how to approach the conversation:


-
SKILL 1: AFFIRMATION AND VALIDATION

-
SKILL 2: REFLECTION

-
Example of reflection:

-
SKILL 3: ASK-OFFER-ASK

-
Skill 4: Summarise and next steps

-
Students mustViewHere are three role play scenarios for you to practice or to reflect on. It is a chance to put into practice some of the techniques you have learned about. You could do these with a friend or colleague in role; or just practice out loud what you might say to the patient in the cartoon strip

-
Students mustMark as done
-
Students mustMark as done
-
"THIS APPROACH TAKES TOO MUCH TIME!"
You may have noticed that the approach we are promoting here seems to take longer than the more directive approach. Well....yes it usually does. But is it worth spending a little extra time to really address patients' concerns and help them feel better placed to make a decision?
The alternative is often a very brief conversation which doesn't use these sort of techniques - which is less effective at helping patients come to a decision, and which you may have to have repeatedly. Not to mention the risk of losing trust and respect with your patients, which can be long-lasting.
-
-
Students mustMark as done
SIDE EFFECTS OF COVID-19 VACCINES
It is important to let patients know about common side effects as well as possible benefits of the vaccine.

This information is from the NHS:
The COVID-19 vaccines approved for use in the UK have met strict standards of safety, quality and effectiveness.
They can cause some side effects, but not everyone gets them.
Any side effects are usually mild and should not last longer than a week, such as:
- a sore arm from the injection
- feeling tired
- a headache
- feeling achy
- feeling or being sick
More serious side effects are very rare.
Find out more about COVID-19 vaccines safety and side effects
-
Students mustView
Concise evidence-based answers to common Covid vaccine concerns, available in many languages. From the Islamic Medical Association
[NB They use the term "myths", but feedback from our community suggests that this can seem dismissive of peoples' genuine concerns. When speaking with patients, it is probably more helpful to refer to them as "concerns" or "rumours" rather than myths]
-
Students mustView
After you have browsed the collection of videos and articles representing the views of the vaccine hesitant, record a short video in which you offer people reliable information using the following structure:
1 Argument or concern against vaccination.
2 Counter-argument, supporting vaccination
-
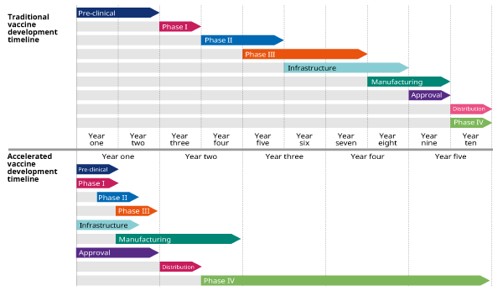
Source; WHOExample: addressing a common concern
How can the vaccine be safe if it was developed so quickly?
Lots of collaboration!!
Two key facts:
1. Process is usually done in sequence (requiring separate funding and ethical approval at each step). This time many preparatory steps were done in parallel
2. This was a highly prevalent infection – so lots of people were at risk. That made it easier to test in trials
-
Students mustView
Evidence-based information about the Covid-19 Vaccine, from the NHS
-
Experts from Johns Hopkins Medicine review some common myths circulating about the vaccine and clear up confusion with reliable facts.
-
-
Students mustViewThere is lots of information online that is poor quality, incorrect, false (misinformation), deliberately deceptive or potentially harmful (disinformation). So it is really important to have the skills to evaluate anything you find.This interactive page introduces three useful techniques for evaluating the information you meet online. You may also find them helpful when talking with patients about how to judge the reliability of their information sources:1 Lateral Reading2 S.I.F.T and3 Fact-checking
-
-
-
PATIENT FOLLOW-UP

-
We would really appreciate your feedback about the module if you can spare a few moments to say what you liked and what we could do differently. Thank you so much.
-